MELASMA
Approaching MELASMA
Dr Chiranjiv Chhabra and Dr Priyanka Aggarwal focus on treating melasma with energy-based devices and lasers.

M elasma is a dysregulation of the homeostatic mechanisms that control skin pigmentation and excess pigment. Treatment approaches are topical and oral medications, chemical peels and laser and light therapy. Several types of energy-based devices have been studied for melasma treatment. A range of different lasers had been tried in treating melasma, with Q-switched Nd-YAG laser (QSL) being the most common one. Recently, laser toning or low-fluence, multi-pass technique has become popular. Intense pulsed light, low-fluence Q-switched lasers, and non-ablative fractionated lasers are the most common lasers and light treatments that are currently performed. The use of non-ablative fractionated laser treatments compared with other laser and light options may result in slightly longer remission intervals. Picosecond lasers, fractional radiofrequency, and laser-assisted drug delivery are promising future approaches to treat melasma. The goal of this review is to summarise the efficacy and safety of the most commonly used laser and light therapies to treat melasma and provide recommendations for treatment on the basis of the reviewed information.
TREATMENT STRATEGY
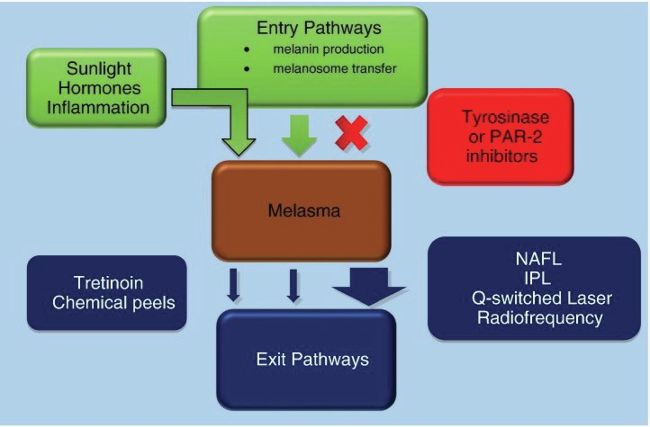
The treatment regimen of patients with melasma typically starts with the management or elimination of risk factors, strict ultraviolet sun protection, and topical lightening formulations. Topical treatments may temporarily improve the skin but the condition often returns. The principles of therapy include the inhibition of pathways that synthesise melanin, decrease of melanosome transfer from melanocytes to keratinocytes, and acceleration of pathways to remove melanin.
TOPICAL AGENTS
The current first-line treatment for melasma is topical agents. The major group of topical agents to be considered are those that disrupt the enzymatic processes of pigment production within melanocytes. Tyrosinase is the rate-limiting enzyme in the melanin production process that converts L-tyrosine to L-3,4-dihydroxyphenylalanine (L-DOPA) and is the major target for many of these agents. Melanin is synthesised through a series of steps and converts the base precursor tyrosine to DOPA and then to dopaquinone, which is converted to dopachrome and eventually to eumelanin. These types of treatments include hydroquinone (often used in combination with tretinoin and a topical steroid), arbutin, azelaic acid, and kojic acid. Ascorbic acid is also another inhibitor of melanogenesis through its antioxidant effects and interaction with copper ions in the tyrosinase active site.
Other targets for intervention in the melanin synthetic pathway include the interaction between keratinocytes and melanocyte. There are several botanical agents such niacinamide and soy that act through protease-activated receptor-2 (PAR-2) and inhibit the transfer of melanosomes to the surrounding keratinocytes. Serine protease inhibitors, lectins, and neoglycoproteins also affect this pathway.
Improving skin turnover is another therapeutic route for the treatment of melasma. Agents that accelerate skin turnover include glycolic acid, linoleic acid, lactic acid, retinoic acid. Certain fatty acids such as linoleic or -linoleic acid may induce the degradation of tyrosinase.
Topical treatments may be unsatisfactory because of a lack of response, slow rates of improvement, or adverse events such as pseudoochronosis with hydroquinone or skin irritation, erythema, and post-inflammatory hyperpigmentation
CHEMICAL PEELS
The addition of chemical peels to a topical treatment regimen is secondline treatment as peels help accelerate the elimination of pathways for melanin. Superficial peels such as glycolic acid, Jessner, and retinoic acid are typically selected because they tend to have the least risk of complications and exacerbation of pigmentation if there is too much inflammation or irritation. Peels have been shown to be effective, especially when used in a series of treatments. Chemical peels may cause melasma rebound or PIH due to irritation or inflammation.
LASER-AND LIGHT-BASED TREATMENTS
Laser and light therapy represent an alternative third-line approach to treat melasma and may be particularly beneficial for patients with melasma that is refractory to topical therapy or chemical peel regimens, or when a patient wishes for an accelerated pace of improvement. Analogous to chemical peels, these modalities accelerate the removal of pathways for melanin but do not target the melanin production itself. Furthermore, they present a risk for PIH or a rebound melasma flare. Optimal treatment management of difficult cases should include a combination therapy whereby a topical regimen inhibits melanin production and/or melanosome transfer and a procedure accelerate melanin removal.
LASER-AND LIGHT-BASED TREATMENT
Using laser therapy to trea melasma has become an alternative to the more common treatments with topical creams and chemical peels, especially for patients with refractory cases. A multitude of different laser therapies have been studied in numerous clinical trials to date and a vast range of efficacies and adverse events have been demonstrated. Frequently, the outcomes of these studies are reported through physician-graded assessments or changes in the melasma area severity index (MASI). The five broad categories of laser and light therapy include intense pulsed light (IPL), Q-switched lasers, picosecond lasers, non-ablative fractionated resurfacing lasers and ablative fractionated resurfacing lasers. The objective of this review is to comment on both the efficacy and safety of the most commonly used laser and light therapies for the treatment of melasma as published in the current literature and present new device-based treatment options that are in development for patients with melasma.
INTENSE PULSED LIGHT
IPL therapy uses a flash lamp light source that emits noncoherent light with wavelengths between 515 nm and 1,200 nm. Filter sets allow for the targeting of selective chromophores (melanin vs haemoglobin) and has been used to treat various pigmentary disorders. Its potential advantage over laser therapy is that it uses a spectrum of wavelengths that allow for the penetration of various levels of the skin and target both epidermal and dermal melasma simultaneously. The pulse duration of IPL is in the millisecond range and provides greater thermal diffusion and a reduced chance of thermal-related post-inflammatory pigmentation. The size of the IPL head is larger than most laser spot sizes, which allows for the rapid treatment of large areas.
Q-SWITCHED LASERS
Q-switched lasers produce high intensity laser beams with very short pulse durations. The speed of a Q-switched laser pulse is approximately one million times that of an IPL pulse. Q-switched lasers that target melanin are available in multiple wavelengths including ruby (694 nm), alexandrite (755 nm), and neodymium-doped yttrium aluminium garnet (Nd:YAG; 532 nm or 1064 nm). Because these lasers are standard therapies for the removal of birthmarks, solar lentigines, and tattoos, they are expected to be effective for the treatment of patients with melasma as well.
A new variant of Q-switched laser use called sub-thermolytic Q-switched uses low-fluence treatments largely utilise the 1,064 nm wavelength, which penetrates deeper into the dermis and leaves the epidermis relatively spared. The treatment of patients with melasma with subthermolytic low fluences is based on the theory that the pigment disruption takes place through a photoacoustic mechanism that breaks apart the pigment only and spares the keratinocytes and melanocytes from destruction. However, there is often some degree of damage that accompanies subthermolytic Q-switched treatment, but this damage is reported to be less than that from traditional photothermolytic treatment.
QSL at 1064nm is the most commonly used laser in melasma treatment because of its deeper penetrating properties and safety in pigmented skin.
In 1999, Goldberg and Metzler proposed a concept of laser toning. They used multiple passes of low-fluence QSL to improve photoaged skin. Studies showed that the Q-switched laser was effective at removing melanin particles in the basal layer.
Laser toning or low-fluence, multipass technique is a popular method for treatment of refractory melasma. The term “laser toning” originates from the improvements in skin tone that result from the use of the laser.
THE PROCEDURE
The procedure of laser toning is relatively simple:
• Choose 1,064-nm wavelength of QSL.
• The largest spot, 6–10 mm available on the system, should be chosen.
• The fluence chosen will be in between 0.8 and 2 J/cm2 depending on the spot size of the laser. The starting fluence is chosen according to the spot size available with system and colour of melasma. For a spot size of 8–10 mm, the fluence range should be between 0.8 and 1.4 J/cm2.
• The handpiece should always be held perpendicular to the skin.
• Frequency should be 5–10 Hz.
• There should not be an overlap of more than 10–15 per cent between the two pulses.
• The endpoint of the treatment will be faint erythema or three to four passes (if there is no perceptible erythema).
• The darker the melasma, lesser will be fluence and vice versa.
• Aminimum of 10–12 sessions with a weekly interval or once in 15 days should be conducted. The authors use it once in 15 days because we have found that once-a-week treatment increases the chances of mottled hypopigmentation in
Indian skin.
• After procedure, broad-spectrum sunscreen is used. Patients can resume their topical after 1–2 days after procedures.
MECHANISM OF ACTION
The traditional QSL treatment is based on the principle of selective photothermolysis, which uses a high fluence to destroy the pigmentcontaining cell.
The collimated flattop beam, large spot size, ultrashort pulse duration, low-fluence, and multiple passes of QSL are believed to cause minimal damage to the melanocytes, but it can destroy the melanosomes and melanin granules within melanocytes and keratinocytes but keeping the cell membrane and nucleus intact, thus avoiding cell death. This mechanism is known as “subcellular selective photothermolysis”. The long dendritic processes of hyperactive melanocytes are cut-off (dendrectomy), and there is functional downregulation of melanocytes, which results in the production of a reduced number of melanosomes.There is a less chance of exacerbation of melasma because is no cell death and heating of skin is kept to a minimum.
Melasma can be an epidermal, dermal, or more often of mixed type. Using large spot size and longer wavelength, the depth of penetration can be increased even with less fluence. This helps in targeting the deeper component of melasma and melanophages in dermis. It is mandatory to use a system with top-hat fluence for laser toning. The top-hat beam distributes the fluence all along the spot, avoiding the hot spot as in Gaussian beam lasers. Laser toning uses low-fluence and multi-pass technique as against the single-pass high fluence treatment of selective photothermolysis. Using multiple passes, the melanosomes are heated slowly and destroyed, but the cell membrane and nucleus of the cell are kept intact because of which the cell death is avoided.
Laser toning is found to be effective in the treatment of melasma. It can effectively reduce the size, homogeneity, and pigmentation of melasma lesions. Various studies in the past few years confirmed these findings.
COMPLICATIONS
Safe and effective laser toning is not free from complications. Reported complications from laser toning include pain during the procedure, rebound of melasma, hyperpigmentation, guttate leukoderma, physical urticaria, acneiform eruption, minute petechiae, whitening of fine facial hair, and herpes simplex reactivation. Most of these complications are mild and self-limiting except hypo- or depigmentation.
Relapse and worsening of melasma have been reported after toning. The risk factors for relapse may be high cumulative fluence and small spot used for the treatment. Hofbauer Parra et al studied 20 Latin American patients with laser toning and reported significant improvement in all patients with minimal side effects. However, 81 per cent of their patients’ skin condition relapsed or worsened after discontinuation of treatment. The high relapse rate was also reported in other studies.
Confetti-like hypopigmentation or punctate leukoderma is the most distressing complication of repeated lowfluence laser therapy. It can develop after several sessions or as early as the second session. The cumulative dose of repetitive laser treatment may affect melanocyte function, resulting in the development of hypopigmentation.
Laser-toning-induced hypopigmentation in patients with melasma generally does not respond well to treatment. Such hypopigmentation often persists for many years despite a variety of topical and phototherapy treatments. Various treatment options such as topical steroids, topical tacrolimus, narrowband UVB therapy, and TCA CROSS have been tried with limited success.
CONCLUSION
Laser toning has become an extremely popular procedure in recent years. Authors have used laser toning in those patients who failed to respond all standard lines of treatment, and got mixed results. In the authors experience, laser toning with 1,064-nm QSL with a spot size of 10 mm, fluence of 0.85–1.2 J/cm2, 10-Hz repetition rate, multiple passes (average 3–4) performed once in 15 days for a total of 8–10 sessions yield good results. The chances of hypopigmentation are minimal with the use of 10-mm spot size and minimal overlap of pulses. The authors also combine either dual toning (quasi-long pulse and laser toning) or gold toning (585-nm QSL with laser toning in selected cases with reasonably good outcomes.
NON-ABLATIVE FRACTIONATED RESURFACING LASERS
Fractional resurfacing can be broadly categorised into non-ablative fractional laser (NAFL) and ablative fractional laser (AFL). NAFL devices target watercontaining tissues but create columns of coagulative damage within the dermis that are below the ablative threshold. The stratum corneum is intact throughout the treatment and a visible wound does not occur. The most common affect immediately post-treatment is erythema and swelling. Four NAFL wavelengths are used including 1,440 nm, 1,540 nm, 1,550 nm, and 1,927 nm. NAFL at 1,440 nm, 1,540 nm, and 1,550 nm utilises midinfrared wavelengths that bypass the epidermis and penetrate from the dermal-epidermal junction to the midreticular dermis (maximum depth approximately 1,500 microns) to induce neocollagenesis and remodeling. The transepidermal elimination of these microthermal treatment zones in the weeks post-treatment facilitate the removal of dermal melanophages and be the main mechanism for melasma improvement (Hantash et al, 2006). NAFL at the 1,550 nm wavelength has been approved by the FDA since 2005 for the treatment of patients with melasma. Erythema, swelling, and pain are common with NAFL at 1,440 nm, 1,540 nm, and 1,550 nm but these are short-term side effects that typically last for 3 to 10 days and overall, this treatment is considered a low downtime, fast recovery procedure.
NAFL treatment in general seems to offer a more durable response in comparison with IPL and Q-switched laser treatments especially when patients continued treatment with a topical anti-tyrosinase cream before and after treatment. Although there is recurrence with all NAFL treatments, the data suggests that recurrence occurs between three and six months, whereas IPL and Q-switched laser recurrence tends to occur before three months. The number of treatments that are required for a benefit with NAFL seems comparable with those that are reported for IPL (approximately four) and approximately 50 per cent fewer treatments compared with Q-switched laser therapy, which is often done weekly for eight to 10 treatments.
NAFL with the 1,927-nm device may offer more effective single treatment response compared with all other devices although the type of melasma (epidermal or dermal) that 1927-nm NAFL is best suited for has yet to be determined. The benefit of NAFL is its ability to treat a wider range of skin types including Fitzpatrick skin types III–VI compared with IPL and Q-switched lasers, which should only be used on skin types I–III. Lastly, because of the fractionated mechanism, NAFL may also be better at blending melasma with the surrounding unaffected skin.
ABLATIVE FRACTIONATED RESURFACING LASERS
Ablative fractionated resurfacing lasers (AFL) such as CO2 lasers and erbium:YAG lasers have been reported for the treatment of patients with melasma (Morais et al., 2013). The CO2 laser emits a 10,600- nm wavelength, which is strongly absorbed by water in the skin cells. The penetration depth is dependent on the water content and independent of either melanin or haemoglobin. A fractionated approach decreases the amount of epidermal injuryresulting in fewer side effects and less risk of dyspigmentation. It has also been suggested that the microscopic injury zones that are caused by fractionated ablation allow for the transport of necrotic epidermal debris including melanin through the DEJ. Early results with a nonfractioned CO2 laser highlighted the risks for PIH.
The cutaneous absorption of the Er:YAG laser energy by water (2,940 nm) is 10-fold efficient than that of the carbon dioxide laser and allows for more superficial tissue ablation but with minimal thermal damage. Furthermore, clinical improvement as assessed by dermatologists who were blinded to the treatment showed that only 15% of patients sustained improvement that was greater than 50% after four months of follow-up (Wanitphakdeedecha et al, 2009).
PICOSECOND LASERS
Recent innovations in laser design have introduced a new class of lasers that generate picosecond-domain pulses. Shorter laser pulse durations result in pigment fragmentation that is more a result of photoacoustic than photothermal effects. Therefore, it may be more efficient at pigment removal without inducing thermal damage to surrounding tissue. This thermal damage seems to be the greatest drawback of conventional Q-switched laser treatment for patients with melasma and likely the cause of the high PIH rates after treatment.
Picosecond lasers are available with laser outputs of 532 nm, 755 nm and 1,064 nm. Thus far, however, no data has been published about their efficacy in patients with melasma either using settings for benign pigmented lesions like solar lentigos or at low fluence treatments that are analogous to low fluence Q-switched laser treatment. More recently, fractionated picosecond handpieces have been developed for the purpose of resurfacing and rejuvenation they work via photoacoustic mechanisms, they may present a new treatment modality that is suitable for patients with melasma.
OTHER LASER TREATMENTS
Other types of laser therapy include pulsed dye lasers (PDL; 585 nm) and copper bromide (CuBr; 511-578 nm) lasers, which are thought to work by targeting the vascular component of melasma. However, targeting vascularity as a treatment for patients with melasma has not shown a significant benefit.
FUTURE ROLES OF LASERS OR OTHER DEVICES IN THE TREATMENT OF MELASMA
In future, lasers or other devices may contribute to the treatment of patients with melasma not only by targeting pigment directly but by facilitating the delivery of topical medications, which is a technique that is known as laser-assisted drug delivery (LADD). Currently, most topical therapeutic treatments have poor bioavailability due to the difficulty to penetrate the skin barrier. With LADD, CO2 or Erb:Yag ablative lasers create a matrix of transepidermal channels that provide direct access to deeper layers of the skin and facilitate cutaneous and transcutaneous drug delivery. By manipulating the density and depth of these channels, it appears possible to manipulate the amount of drug that is absorbed, the delivery rate, and the drug biodistribution, which may lead to improved clinical efficacy. LADD with ablative lasers has the largest body of evidence for efficacy and particularly as a pre-treatment to enhance the penetration of aminolevulonic acid or methylaminolevulinate prior to photodynamic therapy. However, studies are ongoing to assess the delivery of numerous substances with multiple laser modalities. At least one recent study has shown the potential of nonablative fractional lasers to deliver small- and macromolecule. The hope is that LADD may offer a more effective way to deliver medications especially for the dermal type of melasma for which topical delivery seems to be out of reach and has limited success.
Analogous to LADD, microneedle (MN) technology creates micronsized pores through the epidermis to facilitate the transport of therapeutic molecules into the epidermis. Instead of a laser, microneedling uses a roller device with hundreds of micron-length needles that create an array of pores to act as aqueous transport pathways through the stratum corneum. These micropores are larger than the pores that are created by LADD and may permit the transport of hydrophilic macromolecules, peptides, deoxyribonucleic acid, and small interfering ribonucleic acid constructs (Donnelly et al., 2010). MNs are now exploited in the cosmeceutical industry as a means to disrupt the skin cell architecture and induce elastin and collagen expression and deposition. They are also used as a means to deliver cosmeceutic molecules across the skin (McCrudden et al., 2015).
Radiofrequency (RF) devices have become much more popular in the last few years due to their efficacy in tightening and rejuvenation, high safety profile, and minimal post-treatment recovery time. RF devices create an electrical current that, when in contact with tissue, encounters impedance and creates heat energy that in turn stimulates collagen production. Furthermore, RF technology is independent of pigment; therefore, it is safe to use in patients of all skin types and has a low risk of hyperpigmentation unless too much bulk heating occurs or arc burns are created on the surface of the skin from inadequate contact with the skin.
Laser and light therapy for the treatment of melasma is best-suited for patients with refractory melasma who failed with topical treatment or a series of chemical peels. Topical therapy takes at least three months or longer to see skin lightening and those patients who are interested in a more rapid response could consider laser and light therapy. A proposed therapeutic ladder for melasma is indicated in Table 1. Counselling prior to treatment should disclose that procedural treatments are not cures for melasma but studies have shown that lightening of the affected skin can occur after a series of treatments. Patients should also be counselled on the likelihood of recurrence, PIH, and rebound hyperpigmentation. A significant number of patients (approximately 50 per cent) will have recurrence to some degree within three to six months of their laser- and light-based procedure regardless of the type of device used.
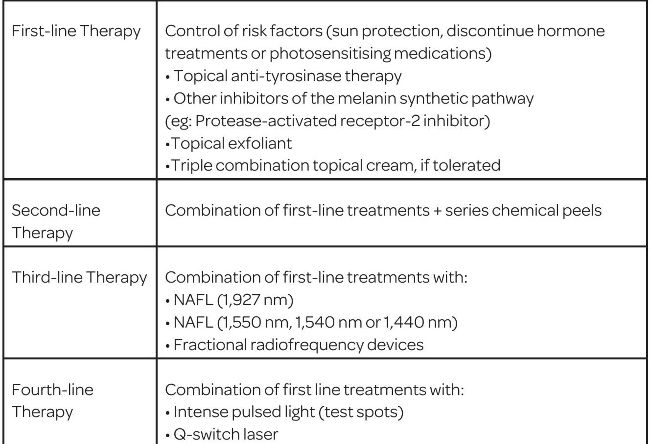
Table 1 : Proposed therapeutic ladder for melasma
NAFL, nonablative fractional laser.
The goal of melasma therapy is to limit the entry pathways and increase the exit pathways so that there is net loss of pigment. Once the desired amount of lightening is achieved, the next step is to find a maintenance regimen that keeps the entry and exit pathways in equilibrium. This may involve control of risk factors, topical treatments, sporadic procedural treatments, or a mixture of these techniques. The proper choice of procedural treatment will have to integrate the patient’s melasma-specific medical history, Fitzpatrick skin type, melasma type (epidermal, mixed or dermal), other forms of hyperpigmentation that may be present within the melasma sites, and preand post-procedure topical therapy and maintenance treatments.
The patient’s medical history and current and prior procedural treatments for melasma are important. If no preventative treatment or topical lightening regimen is used, a treatment regimen should be initiated at least two to six weeks prior to the procedure treatment. One unifying concept in all the laser and light therapies that have been tested so far is the synergism between topical anti-Tyrosinase treatment and the laser and light procedure. In general, pre-treatment and posttreatment topical regimens in conjunction with laser and light treatment helps reduce the risk for rebound hyperpigmentation, post-inflammatory pigmentation, and increases the longevity of the lightening effect on melasma. To control risk factors for melasma by use of avid sun protection and avoidance of hormonal triggers is also important to maintain the benefits from laser treatment. Understanding what the patient has experienced in prior procedural treatment failures will help narrow the field of alternative options to discuss.
Patients with lighter-coloured skin types (Fitzpatrick type I-III) will generally have less risk for PIH or post-inflammatory hypopigmentation. They may be more tolerant of any of the laser and light treatment options that are presented above. Patients with darker skin types (Fitzpatrick type IV-V) will likely have a higher risk with Q-switched lasers, and IPL and NAFL treatment options may have a higher benefit-to-risk ratio and be better at blending the melasma-affected areas with normal skin.
Most of the clinical studies for laser- and light-based treatments are not categorised by type of melasma (epidermal, mixed, or dermal). For some procedures such as NAFL, knowing the type of melasma may be beneficial because the different NAFL wavelengths penetrate to different depths within the skin that are more likely to be effective. For instance, NAFL at 1,927 nm penetrates just under the stratum corneum to a depth of 200 microns, NAFL at 1,440 nm works from the DEJ to a depth of 300 micron, NAFL 1,540 nm from the DEJ to725 microns, and NAFL at 1,550 nm from the DEJ to 1,350 microns (Fig. 2A). The depth for each device is adjustable by changing the fluence.
Epidermal melasma is likely more responsive to NAFL at 1,927 nm (Fig. 2B) whereas dermal melasma is likely more sensitive to NAFL at 1440-nm, 1540-nm, and 1550-nm wavelengths. As non-invasive imaging techniques such as reflectance confocal microscopy, electrical impedance spectroscopy, or optical coherence tomography improve, a better idea of the depth of treatment needed to treat patients with dermal melasma may become clearer. At this time, most NAFL at 1,440 nm, 1,540 nm and 1,550 nm is done with settings that are focused on the papillary or mid-dermis. Some of the suggested mechanisms for melasma involve dermal extracellular abnormalities. NAFL affects all the substrates within their microthermal treatment zones, unlike Q-switched lasers or IPL that only target pigment itself. Correction of these dermal abnormalities may be one reason why the recurrence rate seems less with NAFL compared with Q-switched lasers.
Studies of laser- and light-based treatments for patients with melasma have shown that a long-term posttreatment maintenance regimen is necessary to slow the recurrence of melasma and minimise rebound hyperpigmentation or PIH. Also, limited studies have suggested that skin immediately post-NAFL or AFL may be in a state that facilitates the delivery of topical medications. To incorporate these findings plus limit any inflammatory cascade from the laser treatment or thermal injury, the following pre- and posttreatment regimens are recommended prior to laser- and lightbased treatments (Table 2, Table 3).
Table 2 : Proposed pre-treatment regimen
Table 3 : Proposed pre-treatment regimen
Topical tyrosinase inhibitors should be applied immediately after the treatment is completed in addition to a high potency topical corticosteroid drug. The topical tyrosinase inhibitor should be maintained at least daily for two weeks and the topical corticosteroid drug should be maintained twice per day for an additional three days. After two weeks, a topical exfoliant such as tretinoin or a topical triple combination cream (antityrosinase, tretinoin, low potency steroid drug) should be used daily. To optimise the benefit of topical therapy, other agents that affect the melanin synthetic pathway such as Par-2 inhibitors should be added to the pre- and post-treatment maintenance regimen. Topical lightening agents may be irritating and the risk of this post-procedure treatment is the balance of irritation from the lightening agents that may result in PIH and the ability to deliver the medication to the depth required for lightening, topical steroids might help balance the irritant effect.
Light and laser therapy is an alternative approach to treat patients with recalcitrant melasma. The current methods are limited by recurrence, post-inflammatory dyspigmentation, and the need for multiple treatments. However, as the treatments transitioned from Q-switched lasers and IPL to NAFL, the recurrence rate and number of treatments necessary to see benefits have decreased. The treatment will continue to evolve as advances in laser or device technologies emerge. Imaging and drug delivery methods can enhance these technologies, and it will be interesting to see how the picosecond lasers and fractional radiofrequency devices will impact melasma treatments.
ABOUT THE AUTHORS:
Dr Chiranjiv Chhabra is the Chief Dermatologist and Director at Alive Wellness Clinics
Dr Priyanka Aggarwal is an Aesthetic Physician at the Alive Wellness Clinics.