Injection protocol to restore contours and vectors
Botulinum Toxin Club’s Dr Harry Singh introduces his new SinghSculpt® protocol
How has the new clinic design positively influenced patient feedback or experience so far?
The new clinic design has had a tremendously positive impact on patient feedback and experience. My patients love it. Many of them take selfies at our designated selfie point adorned with our logo and vibrant artificial flowers. Although I could not use fresh flowers, the bright colours against the pure white backdrop evoke a wonderful feeling. Iam thrilled because this clinic is a dramatic upgrade from my previous one, and so far, no one has complained about the move, location, or discomfort. Moreover, its location opposite Cartel InfraExchange speaks for itself – It is prominently visible from the road. While we have not installed prominent signage yet, our full glass showcase outside does the job. We are planning to add LED lighting eventually, but even without it, our patients easily recognise the place. Additionally, our Google reviews have seen an increase since we moved into this new clinic.
Any clinics that influenced or inspired you while you were designing yours?
Clinics that have influenced me over time include Dr Piyush Borkhatariya’s clinic in Junagadh – surprisingly beautiful for a place it is located in. Also, Dr Chiranjiv Chhabra’s clinic, Alive Wellness, in Delhi; it’s a testament to her pouring her heart into the space. Such places serve as constant inspiration for me. I have a deep appreciation for aesthetics, both in places and people.
What advice would you offer to fellow practitioners contemplating clinic design or renovations to optimise patient experience?
Based on my experience, I would advise fellow practitioners considering clinic design or renovations to enhance the patient experience. Take a moment to visit Cutis or explore our website, www.Cutis.in, where we have started showcasing clinic pictures. This will give you an idea. Remember, investing in degrees and technology is vital, but equally important is decorating your space to offer a great experience.
The SinghSculpt® dermal filler injection protocol aims to restore contours and vectors from the deep structures of the face all the way to the superficial, providing a holistic transformation through the four facial zones of the temple, cheek, mandible, and chin, creating a true S-shaped transformation with style, shape, structure, and support. It was born out of three frustrations I encountered in my clinical practice.
LONGITUDINAL APPROACH
Like many other medical professionals, I was taught to divide the face into horizontal thirds and vertical fifths, then look at each area individually and work on your treatment plan, by dealing with the patient’s main concerns and dealing with each segment of the face independently. There was no explanation of how treating one area would affect other areas, whether to inject medially/laterally or where volume loss would be observed.
Like a good student, I believed in the key opinion leaders (KOLs) and started to implement their advice. Some results were fantastic, and some were very unsatisfactory. I decided then to research more, reading articles, watching webinars, and attending international conferences.
Since the goal of most of our treatments is to hide or slow down the effects of ageing, I investigated in detail how the face ages. I looked at bone loss, fat redistribution, loosening of ligaments and thinning of the dermis. I asked myself how I can impact the complex ageing process in a systematic, organised, predictable and all-encompassing way. The longitudinal/vertical approaches didn’t make sense to me, which led to a shift in treatment away from simply reversing gravitational descent to adopting volumetric approaches to mid-face ageing.
SINGLE LAYER TECHNIQUES
The second problem I saw was that, for the most part, we injected one layer in a particular segment of the face. As mentioned above, the ageing process is multi-factorial and multi-dimensional; therefore, we need to undertake a multi-layered approach. We now know that areas of the face are connected and affect each other, and different depths of the face require different treatment modalities.
There is increasing awareness that structural and volume deficit, as well as vertical descent and ptosis, are critical components of facial ageing. Hence the ’S’ shape is threedimensional on the face.
VECTORING
The final problem I observed was how could we incorporate lifting of the face to provide shape, structure, and support, so I went back and looked at my thread training. If we are placing threads at a certain depth and place to lift the face, using them as vectors and anchors, could we not do the same with our fillers? I found there were certain areas in the face that would allow maximum structural support, which happened to make a ’S’ shape. There are four main facial zones that need support – temples, cheeks, chin, and jawline – which will give the structure and shape the clinician and the patient desires. medial face.
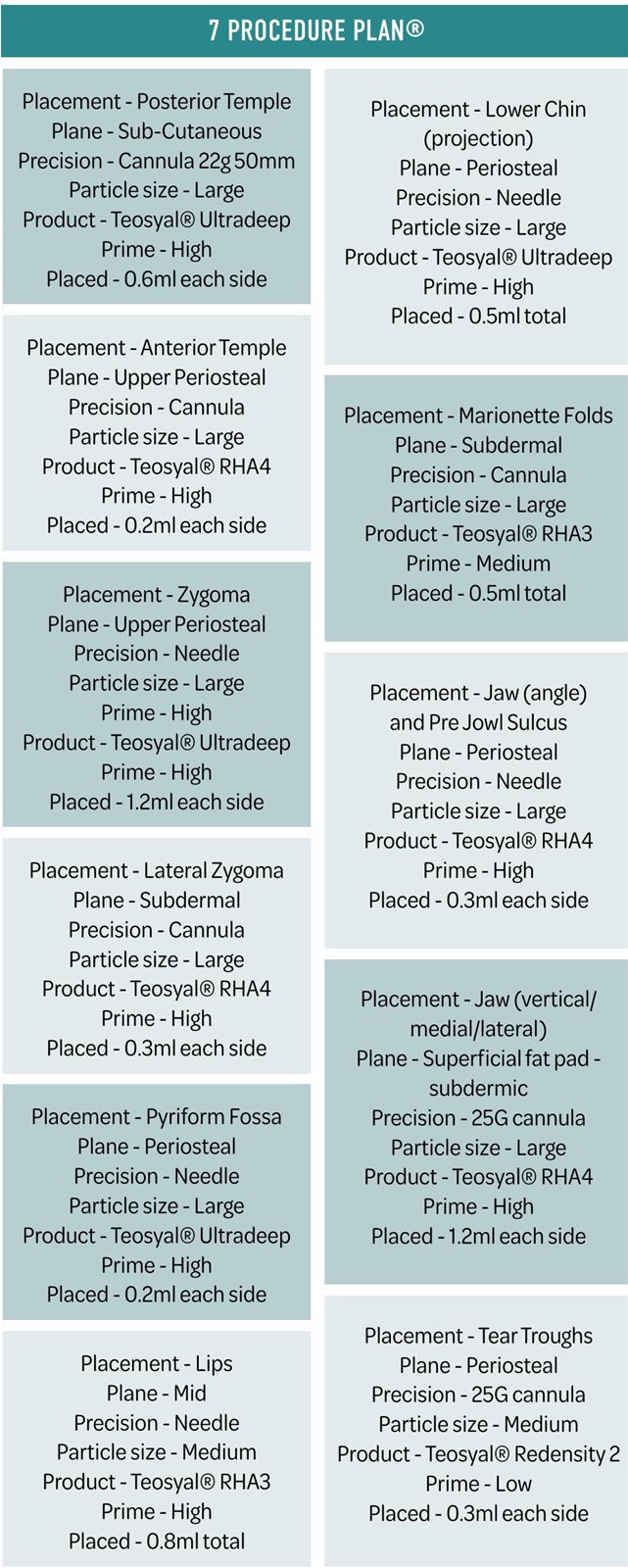
For each area and generally, we will look at seven aspects.
I have looked over my last 20 years of experience and devised a simple way to plan treatment and get predictable results. I came up with certain parameters you must know and plan for before embarking on any treatment. This formed the basis of the 7 Procedure Plan®.
As you will see, it ended • Product up being 7Ps!
• Placement
• Prime
• Plane
• Placed
• Precision
• Particle size
LINE OF LIGAMENTS
The basic idea of the filler injection technique is that whenever addressing the different facial areas/compartments, the order in which one injects and where are crucial in optimising lifting and volumising effects, and to ultimately be more efficient by using less product with similar outcomes as with other filler injection techniques.
As mentioned previously, we will want to use vectoring techniques to our advantage and for this, we need to understand the line of ligaments.
The muscles of mastication are predominately located in the lateral face, whereas the muscles of facial expression are in the medial face. Facial movements are different in the medial and lateral face due to the presence of the line of ligaments.
Separating the mid and lateral face, the imaginary line of ligaments is the connecting trajectory between the four major facial ligaments including the temporal ligamentous adhesion, lateral orbital thickening, the zygomatic ligament, and the mandibular ligament.
Movement in the medial face is directed laterally and movement of the lateral face is directed medially converging at the line of ligaments. The lateral aspect is fixed (no facial muscles present) and the static part, while the medial aspect is mobile (due to the presence of facial muscles) and the movable part. However, passive mobility (due to gravity and age-related changes) is increased in the lateral face, when compared to the medial face.
THE LINE OF LIGAMENTS
Lateral
* Mainly skeleton muscle (SMAS)
* Minimal facial expression muscles and active mobility
* Injecting the stable/anchored tissue to life the face.
Medial
* Facial muscle and superficial fat pad
* Active mobility is affected by the muscles of the facial expressions
* Not a strategic zone to lift the face
* Give projection.
The clinical behaviour of the filler you use depends on where you position it in the face. When you do the lifting, you should never start in the mid-face; but instead, always begin in the lateral face. The best way to respect the proportions and the anatomy is to address the ligaments first, and then contour the face and fill the mid-face according to the patient’s needs.
Injecting laterally, the lateral suborbicularis oculi fat ( SOOF) or fat pad is the most effective area to lift the mid-face. The key is to take advantage of the thick facial ligaments and tense them by placing points very close to the line of ligaments. This creates a very good effect in terms of eye correction and mid-face lifting and can optimise clinical outcomes.
When re-volumising the mid-face, the technique allows the clinician to reposition the facial structures while injecting only a little amount of filler product. After repositioning the fat pads, one can then volumise and contour the mid-cheek and face according to treatment goals.
SUMMARY OF INJECTION TECHNIQUES USING THE LINE OF LIGAMENTS
-Start from the top down, which will reposition the soft tissues to their original location and prevent soft tissue descent, starting with the temples
-Inject laterally first - lateral to the line of ligaments, which preconditions the mid-face, resulting in less product usage. So, first with temples and lateral zygomatic area
-Inject deep first - to restore the bone loss and lay the foundation of support to achieve a more localised effect.
I’d also advise starting with the worst part first, for a couple of
CASE STUDY
The patient is concerned with looking older, sagginess in the lower half of the face and loss of definition.

Before

After
Ageing process reasons.
Full face.We Descent need to of fat make pads, surespecially we use enough markedproduct in jowl areas. to restore symmetry, and the patient will see a bigger difference first.
Diagnosis Volume replacement - minimal Lifting - mid and lower face Definition - lips, jawline Profile enhancement - chin
Treatment planning Making use of the line of ligaments
SUMMARY
This is not a paint-by-numbers tutorial or itemised injection pattern; the SinghSculpt® technique teaches you how to evaluate your patient’s face working through from three dimensions to five dimensions as you learn protocols to help you build structure and shape from the deep tissue to the skin’s surface, creating predictable, natural results.
Remember;
-Know the anatomy to be safe
-Refine your technique to be precise
-Choose the appropriate product for the best result.
REFERENCES
-AkinbiyiT, Othman S, Familusi O, Calvert C, Card EB, Percec I. Better Results in Facial Rejuvenation with Fillers. Plast Reconstr Surg Glob Open. 2020 Oct 15;8(10):e2763. doi: 10.1097/ GOX.0000000000002763. PMID: 33173655; PMCID: PMC7647625.
-Wan D,Amirlak B, Rohrich R, Davis K.The clinical importance of the fat compartments in midfacial aging. Plast Reconstr Surg Glob Open. 2013;1:e92. doi:10.1097/GOX.0000000000000035
- 9Tan M, KontisTC. Midface volumization with injectable fillers. Facial Plast Surg Clin North Am. 2015;23:233-242. doi:10.1016/j.fsc.2015.01.009
-Casabona G, Bernardini FP, Skippen B, et al. How to best utilize the line of ligaments and the surface volume coefficient in facial soft tissue filler injections.J Cosmet Dermatol. 2020 Feb;19(2):303-311. doi: 10.1111/jocd.13245. Epub 2019 Dec 15.
-Freytag L,Alfertshofer MG, Frank K, Moellhoff N, Helm S, Redaelli A, Voropai D, Hernandez CA, GreenJB, Cotofana S. Understanding FacialAgingThrough Facial Biomechanics:A ClinicallyApplicable Guide for Improved Outcomes. Facial Plast Surg Clin North Am. 2022 May;30(2):125-133. doi: 10.1016/j.fsc.2022.01.001. PMID: 35501049.